Written by: Nicole Freeman
As a result of the COVID-19 pandemic, the American people are facing one of the most significant public health crises in United States history. However, the effects of COVID-19 transcend clinical healthcare, as they threaten to undermine our social, political and economic institutions. Although it is difficult to see beyond the limelight of pain and devastation, the pandemic’s exposure of inherent human rights violations toward underrepresented communities within American healthcare may offer hope for revolutionary changes to a corrupt and discriminatory system.
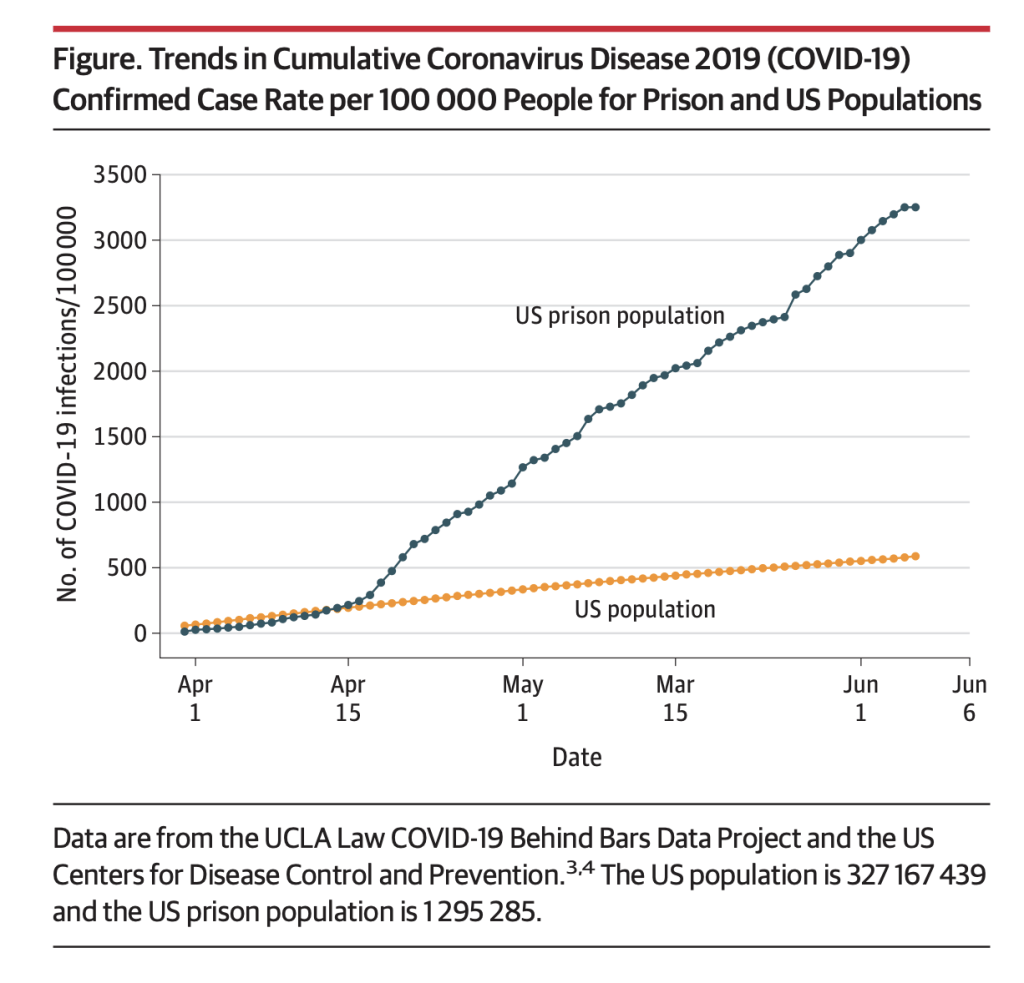
The COVID-19 pandemic has disproportionately inflicted major devastation on marginalized communities. Among these are the socioeconomically disadvantaged, racial minority groups and the incarcerated population — which is notably composed of five times more African American individuals than white individuals. Incarcerated people have been unjustly exposed to the threat of COVID-19. Many of the United States’ largest outbreaks thus far have occurred within the walls of correctional facilities such as jails and prisons. As reported by Johns Hopkins Bloomberg School of Public Health, COVID-19 cases in United States prisons and jails were five and a half times higher and death rates were three times higher than the general population between March 31 and June 6. The lives of the incarcerated are just as important as any other human life; thus, their health must be taken equally as seriously during these threatening and unprecedented times.
Massive disease outbreaks in jails and prisons are nothing new, however. Historically, such facilities have been epicenters of disease transmission. During the 1918 spanish flu epidemic, an account from the San Quentin State Prison in California estimated that over half of the prison’s inmates contracted the flu during the first wave, and the number of inmates reporting sick rose from 150 to 700 each day.
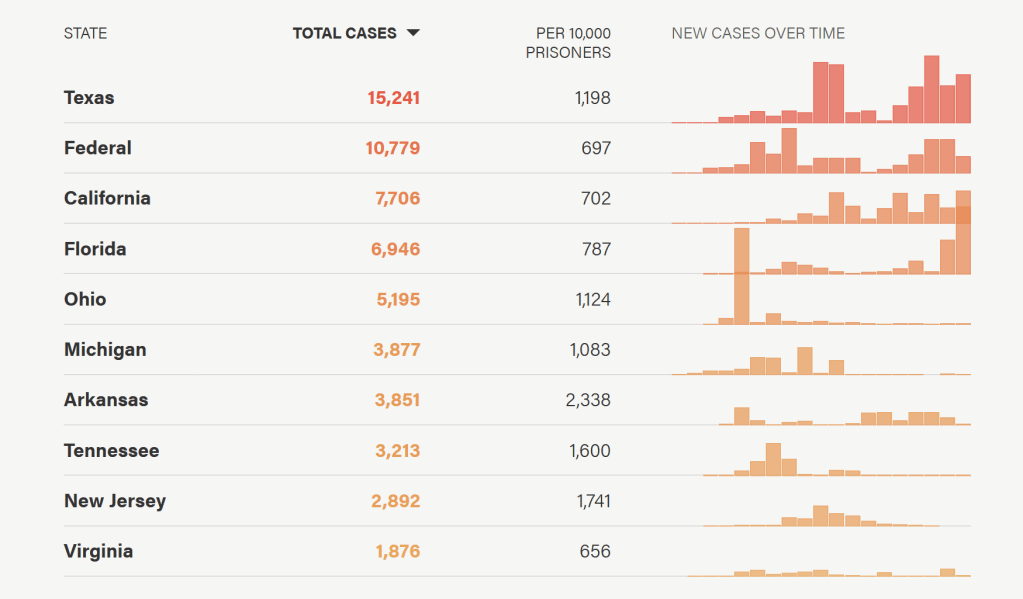
Similarly, according to Human Rights Watch, Ohio’s Marion Correctional Institution experienced one of the worst COVID-19 outbreaks in the United States with over 80% of inmates testing positive as of April 29. Inmates described living in dormitories with over 100 inmates in one — double the recommended capacity. They reported that stacked bunks were positioned only about three feet apart from each other. Additionally, inmates claimed that staff members often ignored the inmates’ reports of symptoms indicating infection.
Although communities across the United States have undeniably faced significant difficulties with preventing the spread of COVID-19, the conditions and practices within jails and prisons have put incarcerated individuals at an increased risk for contracting and spreading the virus that could be minimized through respect of the basic human rights of inmates.
The CDC has recently released thorough documentation of recommendations regarding sanitation, hygiene practices, prevention and testing of COVID-19. U.S. prisons and jails have made efforts to reduce outbreaks by attempting to adhere to these recommendations as well as increasing the number of inmates in solitary confinement and enforcing the use of masks by guards and other workers. However, inmates of the Marion Correctional Institution claim that, at the time of the outbreak, prison staff were not adequately wearing masks, and their facilities lacked clean clothes, soap, and masks for inmates to protect themselves. Inmates also reported that COVID-19 testing was insufficient, as those who reported symptoms would often be moved to solitary confinement and disregarded rather than being tested and provided with proper treatment.
In order to decrease the transmission of COVID-19, a major global focus has been social distancing, which is often a physical impossibility within the prison system. Guards are often required to come in contact with inmates when transporting them, and overcrowding prevents inmates from being able to distance themselves from each other, as they are forced into tight sleeping quarters. Whereas the majority of the American population is able to make the personal decision to stay home to protect themselves and others, inmates are robbed of the ability to safeguard their physical health.
In addition, COVID-19 poses a significant threat to the incarcerated population due to high vulnerability among many inmates. According to a study published by JAMA Internal Medicine, inmates often have poorer health than they would have if they were not incarcerated due to the generally sedentary lifestyles, poor nourishment and unsanitary living conditions. Additionally, the elderly population within jails and prisons has grown recently due to longer sentences. Thus, the vulnerability of incarcerated populations as a result of poor health makes it much more important for additional precautions to be taken to mitigate the impact of the global pandemic. Those serving vulnerable populations outside the prison system — such as within retirement homes — have been taking great efforts to protect the medically fragile individuals. Incarcerated individuals deserve the same respect as all other vulnerable populations during the COVID-19 pandemic.
Access to healthcare is a constitutional right for all inmates under the Eight Amendment’s prohibition of cruel and unusual punishment; however, despite this right, inmates often have limited access to examinations and pharmaceuticals when needed. Incarcerated individuals are unable to continue accessing their previous workforce healthcare benefits and are also ineligible for Medicaid. In addition, inmates in 35 U.S. states must pay additional copayments that go directly towards prison revenue. While the intention of such copayments is to mitigate abuse of medical care, it places an undue financial strain on most inmates whose meager hourly earnings — as low as 12 cents per hour — may not be able to provide for chronic illnesses or other significant health issues.
Though COVID-19 outbreaks within the U.S. prison system — as in any American community — would likely have been unavoidable regardless of proper healthcare and living conditions due to the infection rates of the virus, the scale of such outbreaks has exposed significant violations of human rights within the U.S. prison healthcare system. In order to combat such inequalities, the prison healthcare system could become a non-profit institution separate from the for-profit prison system. Particularly, the co-payments that often deter inmates from seeking treatment ought to be reduced or eliminated entirely, because they do not make up for the spending on healthcare and thus are virtually unnecessary. For example, as of 2017, Virginia facilities spent almost $160 million on healthcare yet only collected about $500,000 from copayments. Such obstacles to care must be eliminated, as they put not only the individual but the entire prison population at risk, especially with regards to a highly infectious virus such as COVID-19.
However, realistically speaking, the current U.S. economy is not in a place that allows such flexibility in monetary profits due to the impact of COVID-19 on employment and government revenue. Therefore, experts have suggested that the optimal solution to mitigate disease outbreaks in U.S. prisons and provide sufficient healthcare to inmates is to reduce overcrowding.
The prison population in the U.S. has quadrupled over the past four decades, forcing many prisons to greatly exceed maximum capacity. Methods for prison population reduction include replacing unnecessary prosecutions of jail time with monetary fines for misdemeanor crimes such as petty theft and possession of marijuana. Additionally, the length of sentences for non-violent crimes should be reduced, because elderly inmates are statistically much less likely to repeat offenses; therefore, reducing a sentence would not pose a significant threat to public safety.
The prison population in the U.S. has quadrupled over the past four decades, forcing many prisons to greatly exceed maximum capacity. Methods for prison population reduction include replacing unnecessary prosecutions of jail time with monetary fines for misdemeanor crimes such as petty theft and possession of marijuana. Additionally, the length of sentences for non-violent crimes should be reduced, because elderly inmates are statistically much less likely to repeat offenses; therefore, reducing a sentence would not pose a significant threat to public safety.
Ultimately, the return to adequate occupancy levels would allow incarcerated individuals to execute their right to protect their health by properly distancing from each other. When the COVID-19 infection curve has flattened and the U.S. economy stabilizes, a transition to non-profit prison healthcare systems would help guarantee proper care for inmates and allow professionals to address the threat of an infectious virus before the situation becomes uncontrollable. As a vulnerable population whose wellbeing is in the hands of the prison system, the incarcerated must be better protected and better served by the healthcare system.
Edited by Sophia Blyth
