
The global pandemic currently ravaging the world began in the Huanan Seafood Wholesale Market in the Hubei Province of China. According to an article in the New England Journal of Medicine, in late December of 2019, Chinese authorities discovered several cases of pneumonia all associated with the Huanan Seafood Wholesale Market in Wuhan. Within one week, on January 7th, Chinese health authorities determined that this cluster of cases was actually due to a novel virus, 2019-nCoV. The announcement that this new species of coronavirus could be transmitted from person-to-person is what should have jolted the general public to treat COVID-19 as a legitimate threat. However, leaders worldwide awaited further news before taking action.
The New England Journal of Medicine also states that within three more weeks, by January 30th, 9976 cases were reported in at least 21 different countries. In fact, the first reported case of COVID-19 in the United States was on January 20th, 2020 in Snohomish County, Washington. From just the first few cases to today, Worldometer displays that we have surpassed 17.7 million confirmed cases worldwide and 4.7 million cases in just the United States as of July 31st, 2020. So where is the vaccine as promised by leaders in the field of science and engineering?
The Step Ladder of Vaccine Development
While many countries may have publicly responded late to the COVID-19 pandemic, enterprises relevant to vaccine development immediately jumped into a worldwide race to produce the first vaccine. In fact, The New York Times argued as early as March 19th, 2020 that a global arms race was underway to formulate the coronavirus vaccine. However, now it has been several months since the coronavirus was first detected, so it is natural to ask “Where is the vaccine?” However, health and science correspondent, James Gallagher explains that vaccines normally take several years to devise, but currently, vaccine development for COVID-19 has been put on the fast track. Still, he states that even the fast track is quite a bit longer than six months. Many research groups have created potential vaccines, but that is just the beginning. Trials must first show that vaccines are safe, and then clinical trials must show that vaccines provoke an immune response to protect people from falling ill. Vaccine production must then be scaled up to develop billions of doses and then the vaccine must prove safety in order to get past regulations. These regulations may seem like unnecessary red tape, but a vaccine that does not work or is unsafe will cause even greater problems. Even on the fast track, Gallagher claims that experts predict the vaccine will be fully developed in mid-2021 at the earliest. Finally, Gallagher asserts that the most difficult part of the vaccine development process will be successfully distributing the vaccine and immunising most of the world’s population.
One specific segment of the vaccine development process that especially extends the timeline is the Clinical Development phase. Within this stage of vaccine development are Phases 1, 2, and 3, which we hear about so often in the media. As early as mid-March, the National Institutes of Health (NIH) released that the Kaiser Permanente Washington Health Research Institute (KPWHRI) in Seattle had begun Phase 1 of clinical trials, but what does that exactly entail? According to The Centers for Disease Control and Prevention (CDC), to enter the Clinical Development phase, private vaccine developers submit an application for an Investigational New Drug (IND) to the US Food and Drug Administration, and once the proposal has been approved, the candidate vaccine must begin its journey through the three trial stages of the Clinical Development chapter. In Phase 1, vaccine developers determine the safety of the vaccine using a small group of subjects. Phase 2 includes several hundred test subjects and aims to determine information about the immune response caused by the vaccine. Finally, in Phase 3, several thousands of test subjects continue to measure the safety and immune response of the candidate vaccine, but vaccine developers are now looking to determine the effectiveness of the vaccine as well. Currently, there are many leading candidate vaccines, which are in various stages across all three phases.
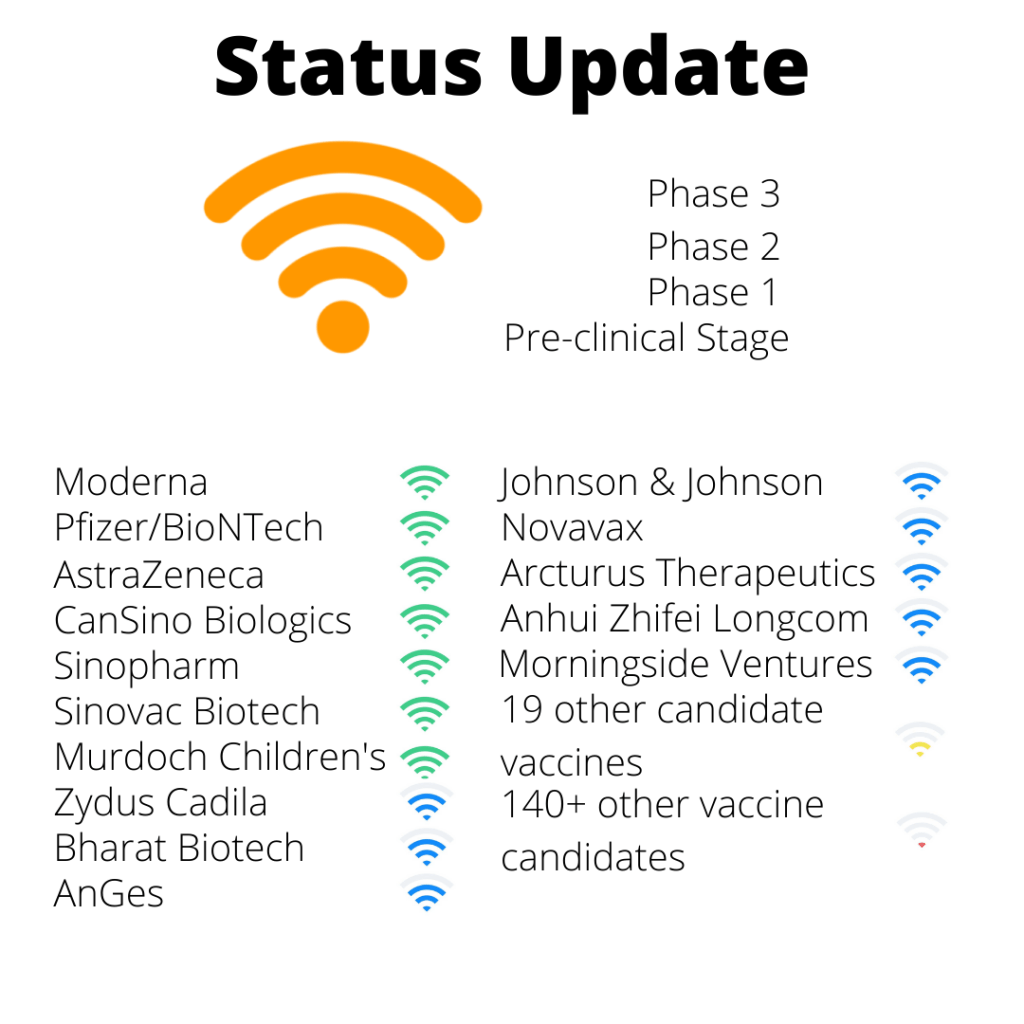
The Current Status
The New York Times reveals that as of July 24th, 2020, the leading candidate vaccines are being developed in the US, China, Europe, and India. American companies Moderna and Pfizer (partnered with German company BioNTech and Chinese company Fosun Pharma) are both entering Phase 3 of clinical trials. Chinese companies CanSino Biologics, Sinopharm, and Sinovac Biotech are also entering or already in Phase 3. The British company AstraZeneca and the Murdoch Children’s Research Institute in Australia have also entered Phase 3. Indian companies Zydus Cadila and Bharat Biotech as well as Japanese company AnGes have entered Phase 2 of clinical development in the search for a COVID-19 vaccine. Many other companies have entered Phase 2 as well, including Morningside Ventures, Arcturus Therapeutics, Johnson & Johnson, Anhui Zhifei Longcom, and Novavax. Jonathan Corum and colleagues with the New York Times also assert that there are 19 other candidate vaccines in Phase 1 trials and over 140 other candidates in the preclinical phase. All of these aforementioned companies are the major players in the worldwide race for an effective COVID-19 vaccine. In fact, NIH Director Francis S. Collins has stated that from the companies currently in Phase 3, including Moderna and Pfizer, he hopes to have an effective vaccine ready for manufacturing and distribution by the end of 2020.
The Joint Efforts of the Public and Private Sectors
One major reason that the vaccine development process for COVID-19 has been able to speed up to its current extent is public-private partnerships. In mid-April, the NIH launched a public-private partnership to place COVID-19 vaccine and treatment development on the fast-track, and this partnership included more than a dozen leading biopharmaceutical companies, the Health and Human Services Office of the Assistant Secretary for Preparedness and Response, the CDC, the US Food and Drug Administration, and the European Medicines Agency. Together, the group developed an international strategy termed “Accelerating COVID-19 Therapeutic Interventions and Vaccines” or the ACTIV plan. By standardizing and sharing preclinical evaluation methods in an open forum, prioritizing and accelerating clinical evaluation of therapeutic candidates, maximizing clinical trial capacity and effectiveness, and creating a collaborative framework to share insights, the ACTIV plan aims to advance vaccine development in the fight against COVID-19.
The government has also aided in COVID-19 vaccine development through direct investment. The federal Biomedical Advanced Research and Development Authority (BARDA) is investing in the leading vaccine developers during clinical trials to ensure enough doses for the American public as well as the quick manufacturing and distribution of these doses. According to a CNBC article from early July, BARDA has distributed $1.2 billion to AstraZeneca to fund research and development and also reserve 400 million doses for the US. BARDA has also awarded $456 million to Johnson & Johnson and $486 million to Moderna. The US government has termed these large investments into a COVID-19 vaccine and the overall fast-track process, “Operation Warp Speed.” Additional beneficiaries include Novavax with $1.6 billion of funding and Emergent Biosolutions with $628 million. Pfizer and BioNTech also announced that the US government reserved up to 600 million potential doses by awarding the companies $1.95 billion to fund research and clinical development. The US government has made plentiful vaccine dose reservations with multiple leading vaccine developers in order to provide the vaccine at virtually no cost for the American public. However, if a company outside the US develops the vaccine, the cost may rise for the American public and there may also be a delay in when the vaccine doses arrive in the US.
Who Receives the First Batch of Vaccines?
Still, once a vaccine is available, new questions are posed: How should the distribution of the future vaccine be prioritized? According to Lena H. Sun with the Washington Post, current discussions and plans for prioritizing the distribution of the COVID-19 vaccine have categorized healthcare workers, other essential workers, and high-risk populations as the highest priority groups. High-risk populations specifically include older adults, residents of long-term care facilities, and people with underlying medical conditions relevant to COVID-19. However, there is much more controversy over who is considered an essential worker. Are cafeteria workers and the cleaning staff at medical facilities considered essential? Are teachers considered essential? Another controversial point is the role that race and ethnicity should play in prioritizing the distribution of the COVID-19 vaccine due to the disproportionate effect of the virus on certain communities of color. Following the high priority categories, there has been discussion about prioritizing children as well as pregnant women. Prioritizing based on location has also been brought up since some regions of the country have been hit harder by COVID-19. Clearly, the story doesn’t end with just the release of an effective COVID-19 vaccine.
With multiple plans in discussion, it is equally important to ask, who gets to decide the prioritization? Statnews writer Helen Branswell stated that in mid-July, the National Academy of Medicine named a panel of US health officials tasked with developing the framework to make the critical decision of who gets vaccinated first. However, the Advisory Committee on Immunization Practices (ACIP) currently exists and already fills this niche, including the creation of the vaccination priority list during the 2009 H1N1 flu pandemic. Moreover, the national government’s Operation Warp Speed has also claimed distribution of the COVID-19 vaccines. Including the opinion of the general public, there are now four entities tasked with making the same decision. Considering that only a small portion of the population will have access to the vaccine at the start, assigning the groups atop the priority list is a critical decision that could impact the spread of COVID-19 while manufacturers and distributors are still working to make the vaccine available to the rest of the population. Even before building the vaccine priority list, these various entities must first decide who gets the final say in prioritization, or they must be in agreement because differing opinions will not succeed in enforcing the priority list.
Handling the Uncertainty
While the scientific community is hunting down a vaccine and the public sector is preparing for mass distribution, what should everyone else do? What should you do? President Trump has stated that the first doses of a COVID-19 vaccine could be available by the end of 2020, but according to Sarah Kolinovsky with ABC News, the Trump administration’s own medical and scientific experts are doubting the possibility of an effective vaccine on such a short timeline. Since vaccines can often take several years to develop, many experts including the Operation Warp Speed lead Moncef Slaoui, Dr. Anthony Fauci, and the former head of BARDA Dr. Rick Bright along with more have stated that even the 12-18 month timeline is formidable. With the current uncertainty on a vaccine any time soon, it is best not to hedge our bets and to play it safe. Social distancing guidelines as well as mask mandates should be thoroughly followed. Avoiding large gatherings and minimizing the number of people we come in contact with will both limit our own chance of being infected and also boost our chances of flattening the COVID-19 curve, at least in our own local community. Like any sporting event, as the audience, we should support the players taking part in the worldwide race for a COVID-19 vaccine in any way that we can. Until there is a COVID-19 vaccine available, all actions to limit the spread of the virus should continue if we want any chance of improving the current state of public health in both the US and the world. It is best to hope for a vaccine, but continue to act as if our own actions are the only vaccine.
Edited by Varshini Odayar
