Written by Segen Ghebrendrias and Zainab Faisal
Racism is often perceived as a force that can reach individuals as soon as their lives begin. The pervasive nature of racism disproportionately favors some communities, preventing them from experiencing life to its fullest. Racial inequalities have been at the forefront in analyzing healthcare disparities plaguing America’s healthcare system. But why do we often ignore the effects of racism on lives that have yet to begin? For many Black infants, why is it that prejudice and policy prevent them from beginning their lives at a healthy weight?
In short, racism is to blame. Racism and racial discrimination are the impetus of the social determinants of health and are a driving force for health disparities. On a macro-level, racism and discrimination can result in residential segregation, where many African Americans live in under-funded areas with little to no access to healthcare. At a micro-level, implicit bias and microaggressions from every day interactions can occur. “As a Black provider, who has experienced racism and seen it in my own family, it is pervasive” says Brittany Edwards, a Certified Nurse Midwife, Women’s Health Nurse Practitioner, and co-investigator for the Patient-Centered Outcomes Research Institute’s collaborative study on preterm births, the EMBRACE study.
A pressing example is the high rate of preterm births and infant mortality among African-American folks. Premature or preterm birth is the birth of an infant before 37 weeks and having a low birthweight of less than 5 lb 8 oz. Breathing problems, brain problems, impaired learning, and heart issues are all complications that can arise from a preterm birth.
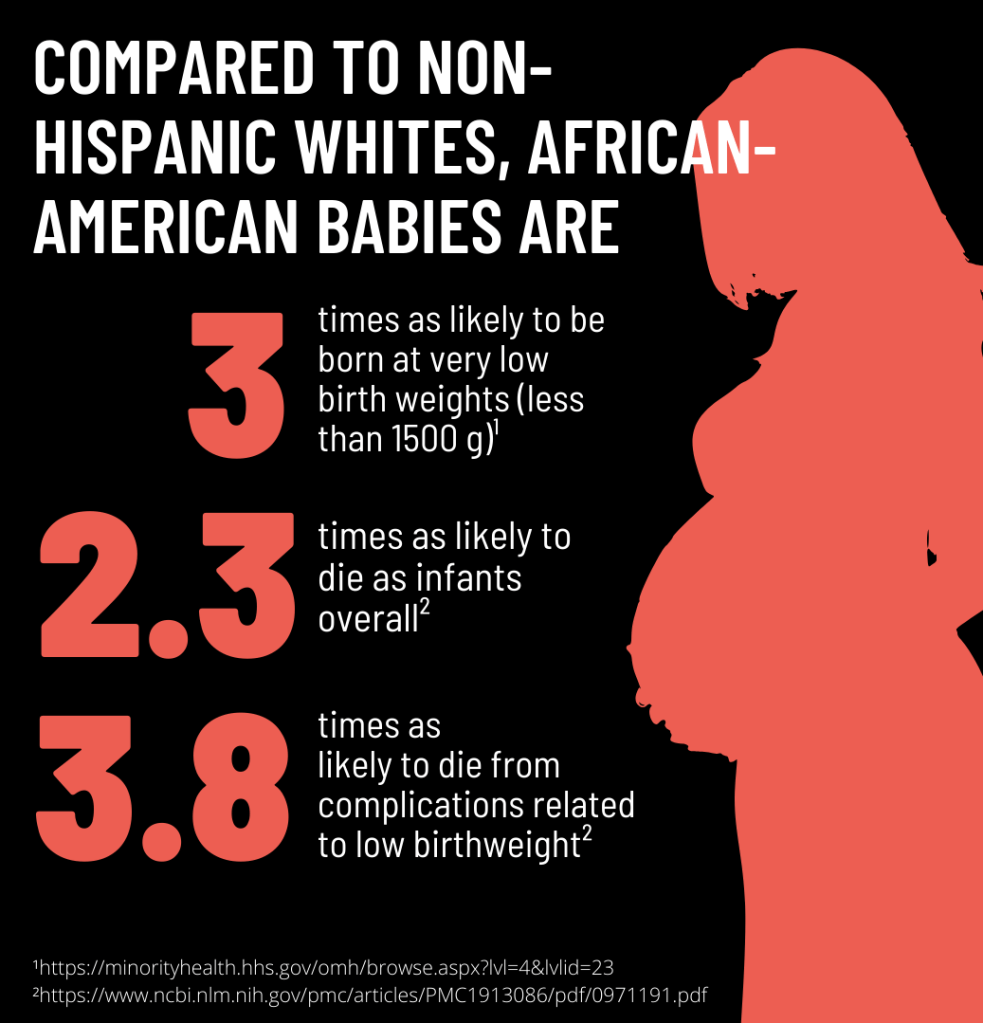
These and other complications can lead to infant mortality within the first year of life. African-American babies are 2.3 times more likely to die within their first year than non-Hispanic whites, and are 3.8 times as likely to die from complications related to low birthweight. Low birthweight is a significant factor in infant mortality and is the leading cause of infant mortality for African Americans. In fact, birthweight is an indicator of the differences in infant mortality between African-Americans and white Americans; the gap in first-year mortality is attributable to the higher rate of Black infants born at very low birth weight (less than 1500 g)— three times that of white infants. These rates alone display an unjustly ignored public health crisis. As Edwards reflects, the
“disproportionate rates of infant mortality in our Black communities is heartbreaking.”
The Genetic Hypothesis
Many scientists have approached this racial disparity with the perspective that genetic differences between racial populations are the major contributors for the gap in birth outcomes. However, Drs. Richard David and James Collins challenge the significance of genetics in racial disparities in infant mortality. If genetics were indeed responsible for these birth weight differences between Black and white Americans, we would see a pattern in birth weights in which Black African women had babies with the lowest birth weights. African-American women would have babies with higher birth weights since they often have European ancestry. Instead, David and Collins found that African-American babies were born with significantly lower birth weights than both African and white American babies. In addition, birth weights for African and white American babies were nearly identical, thus contradicting the hypothesis that this racial disparity is caused by differences in genetics between African and white populations.
Instead, these findings lend themselves to the idea that inherent American social, economic, and political factors could be the source of this disparity. This hypothesis is also supported by the fact that babies of African immigrants experienced heavier birthweights than those of African-Americans, yet the familial birth weights declined after a generation of living in the United States as a minority (David and Collins). These findings suggest that in an attempt to reduce this racial disparity in birth outcomes, we must make an effort to reduce the cumulative adverse effects of a minority status on marginalized populations.
Dr. Richard David, a Neonatal Medicine Specialist at the University of Illinois in Chicago, agrees that genetic research does not hold the key to understanding this gap. “If you just walk into a situation and you see a disadvantaged group of people, it would be perfectly logical to say ‘well, there must be something intrinsically wrong with these people.’ But, if you know the history, and if you have a social system [that disadvantages] people of one particular perceived race, there’s no need to look for genetic explanations.” He also indicates that a genetic hypothesis may perpetuate a view that there is no need for structural and political change since genetic differences cannot be remedied. An attitude of “it’s in their genes. Nothing we do will make it better,” is extremely detrimental to efforts that aim to reduce racial healthcare disparities through social and political change.
Cumulative Experiences of Racism
The African-American experience encapsulates a unique history fraught with psychosocial burdens. Slavery, Emancipation, Segregation, Jim Crow, the Civil Rights Movement—and now, the Black Lives Matter Movement— all portray a history of a never-ending struggle for equality and justice. The compounding experiences among African-Americans is shared historical trauma, and the effects are passed down through behaviors and genetic changes: intergenerational trauma. Messages of how America assails African Americans and continued experiences of racism and discrimination reinforce this race-based traumatic stress.
Encountering racism at school, hospitals, work, restaurants, stores or while seeking housing, warrants an “accept as a fact of life” or “keep it to yourself” perspective. For many African-Americans, internalizing racism and discrimination is their only way of coping with the stress that ensues (Collins et al.). Among middle-class African-American women, exposure to discrimination is far too common, often working in predominantly white spaces, where stress-induced social isolation is grounded in being the ‘token’ Black woman in the workplace. “[African-American women] are thrust into situations where there are mostly white people, and some situations where they’re mostly white men. All of these different factors can influence the number of times per week that they are made to remember what race they are, where they experienced some form of some slight microaggression, or something that contributes to that cumulative accumulation of stress,” David explains.
Transgenerational Trauma and Socioeconomic Status
A toxic environment engendered by racism and discrimination can induce epigentic changes. Epigenetics is the study of how one’s environment affects gene expression through DNA methylation, histone modification, and non-coding RNA. The accumulation of discrimination-induced stress is hypothesized to age an African-American woman’s reproductive system. According to the weathering hypothesis, lifelong or chronic stress causes epigenetic changes that increases health vulnerability, including reproductive health. “This hypothesis could definitely be contributing to poor birth outcomes”, Edwards says. Consequently, according to this hypothesis, African American women who internalize racism and discrimination throughout their life have a higher risk of preterm and/or low birth weight births (Goosby and Heidbrink). Particularly, African American women with severe stress are at an elevated risk for passing cortisol, a stress hormone, through their placenta, which can restrict fetal growth and increase risk for preterm and low birth weight births (Goosby and Heidbrink).
When discussing the impact of chronic stress on the overall health of African-Americans, “it’s important to recognize that this is not unique to looking at the impact of race as a social factor. Social risk factors other than race that behave in the same way, and the main one is, of course, class,” David suggests. He continues by adding that
“in the United States, you will sometimes hear people strongly advocating that the real problem is race and racism, and other people countering that it’s actually just social class and poverty. But in reality, it’s both of these things, and they interact in complicated ways.”
Since the 19th century, studies have shown a social class mortality gradient for various diseases. (David and Collins). Individuals from lower socioeconomic backgrounds are exposed to a variety of risk factors throughout their life history, which can manifest in poor health. Impoverished neighborhoods can negatively impact the health of African Americans by increasing their risk of pollution, childhood crime, discrimination, economic hardships, and other risk factors that collectively contribute to chronic stress and other detrimental effects on adult health (Aroke et al.).
Environmental racism is another significant factor at play. Marginalized populations are disproportionately affected by environmental hazards such as toxic waste, landfills, and other pollution, contributing to health problems that arise from increased exposure to hazardous pollutants. These hazards directly influence the racial disparity in birth outcomes. Elevated levels of lead in the blood of African-American women living in polluted environments are associated with poor birth outcomes (David and Collins).
One misconception is that racial health disparities are only due to inequalities and discrimination within the healthcare system. David counters this by explaining that “only about 10% of the difference in survival outcome between one population and another population can be explained by differential access to medical care. Instead, vast amounts of the difference are due to different life situations such as housing, nutrition, education—access to a variety of similar factors.”
What Now?
“Racist systems will continue to impact us, whether we acknowledge them or not. I believe it is essential for providers of color to create space and community, [to] be aware of how it may impact us throughout the day, and recognize our own biases and triggers,” Edwards suggested.
David offers a similar perspective by suggesting that care providers should be cognizant of their patients’ difficulties: “I mean life is complicated. If people don’t have their own family and environmental systems working well and to their benefit, there are stresses that the doctor or nurse or other provider are poorly equipped to help them with. […] It’s very important to try, as the care provider, to try to offer those things as best you can—if nothing else, as a show of solidarity and understanding.” On top of all the systemic difficulties they already have, it’s the provider’s responsibility to foster an environment of trust and understanding for the patient. Otherwise, failure to acknowledge the social contexts of their patients’ lives is often articulated in patient dissatisfaction and inadequate care. Edwards advocates that “it’s important for providers to be a part of the solution, and recognize the history of mistrust with communities, especially Black communities due to history of medical maltreatment. Patient trust doesn’t develop overnight, it takes time and good reliability. Additionally, having providers that look like their patients help improve communication and build trust.”
Although care providers cannot completely mitigate the risks of their patients at the individual level, it is important to note that social, economic, and political progress can work toward eliminating these health disparities by focusing on the social and environmental differences between populations.
The nature of racism as a “socially generated but physiologically disruptive force” lends itself to the idea that the “physiological consequences created by racial and economic inequality are not inalterable”
Goosby and Heidbrink
However, this requires that the stresses associated with being part of a marginalized population are addressed, and that the physiological consequences of racism are remedied by targeting the underlying systemic and interpersonal mechanisms through which discrimination functions. Otherwise, the pervasive effects of these health disparities will continue to transcend generations and physiologically deteriorate and threaten the lives of the unborn.
Edited By Tyler Schutt
